Go read somebody else's blog (it could save your life)
/
That somebody else is Julia Meade, a resident who attended the 2014 Telluride Patient Safety Resident Physician Summer Camp.
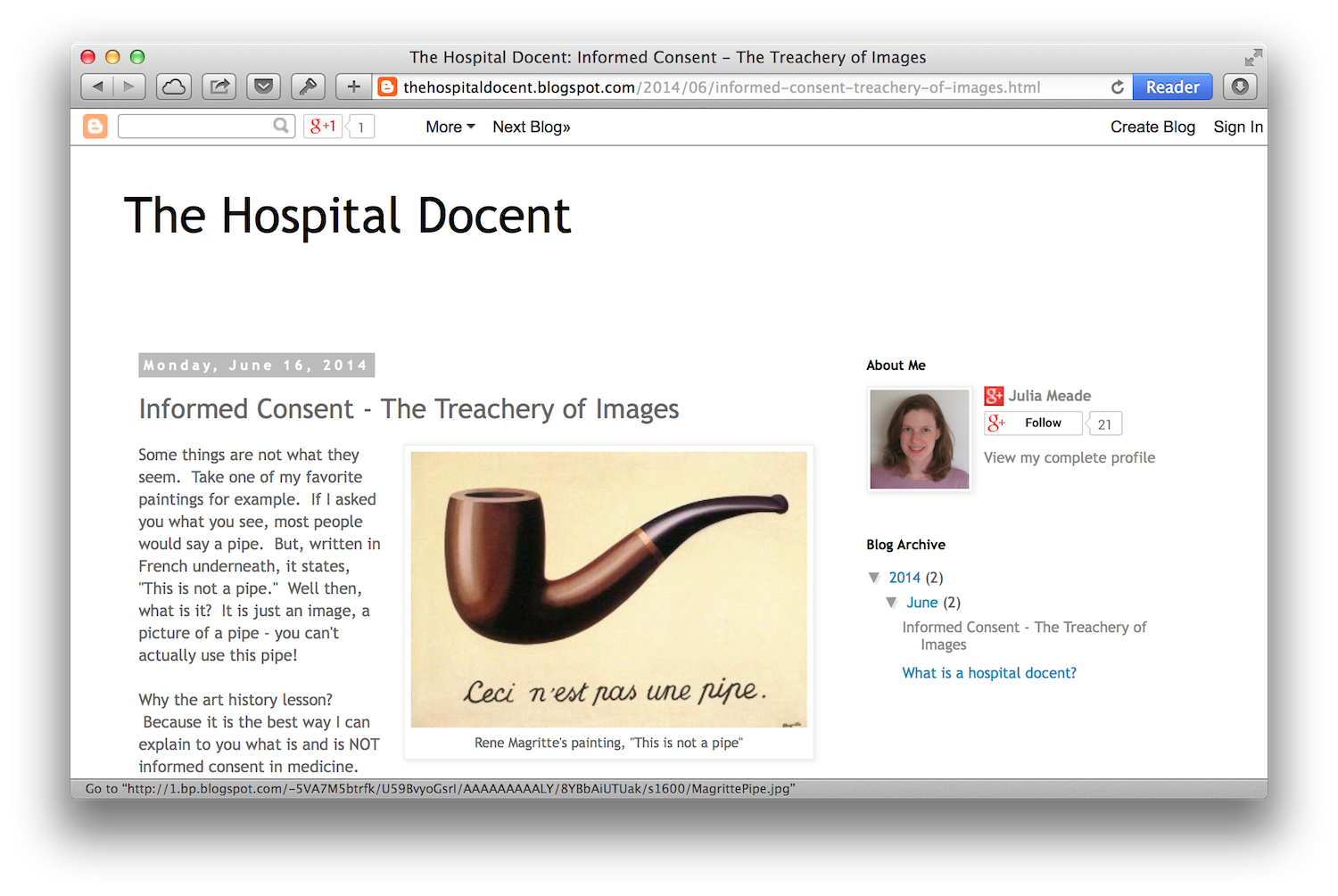
Dr. Meade's new blog, The Hospital Docent, is off to a good start. Her first post is about informed consent, comparing it to a historic painting of a pipe:
Most people, when they think of informed consent, think of a piece of paper they are asked to sign shortly before some procedure or event occurs. It's usually a highly scientific paper with tiny print that most people don't even read before signing. Just like the image of the pipe, it looks like something useful and meaningful, but in reality it's not, it's just a piece of paper.
Dr. Meade then offers five tips for putting the informed into informed consent. Read them here.
I for one am looking forward to a lot of forward-thinking patient-focused writing from Dr. Meade.
Source: Paul Levy.